
FieldStrength MRI magazine
User experiences - August 2020

Edward Steiner, MD, FACR Chief and Medical Director WellSpan Advanced Prostate Care Center York, Pennsylvania, USA
Moving from TRUS biopsies to multiparametric MRI and targeted biopsies guided by fused MRI/ultrasound images benefits high-risk prostate cancer patients at WellSpan York Hospital
Radiologist Edward Steiner, MD, FACR, has collaborated with urologists to set up an alternative patient pathway for prostate carcinoma diagnosis via the use of multiparametric MRI and MRI/ultrasound fusion for targeted biopsies. Particularly when a patient with clinically significant prostate carcinoma had multiple negative TRUS biopsies before, this targeted procedure can help to quite quickly make a confident diagnosis, start therapy and potentially cure patients who have confined disease. This may be life-changing for the patient.
“The power of multiparametric MRI is now not only recognized for exams to identify suspicious lesions, but also expands into guiding biopsies to inform a definite diagnosis”
Using MRI to help identify suspicious lesions in patients with suspected prostate cancer
WellSpan York Hospital, based in York, Pennsylvania, USA, is an advanced specialty care hospital. According to Dr. Steiner, the Chairman of Imaging, the hospital has been using multiparametric MRI and fused MRI/ultrasound image-guided biopsies in prostate cancer diagnosis since mid-2019. He has built a referral base within the five-county community surrounding York and northern Maryland regions.
“Contrary to other techniques, MRI allows for examination of the entire prostate gland with high soft-tissue contrast. Multiparametric MRI allows us to identify suspicious lesions and give these a PI-RADS score [1]. For high-risk lesions, a biopsy can then be performed, guided by MRI images that are fused with ultrasound images in real time. This allows targeting of the lesions that were identified before.”
“Multiparametric MRI allows us to identify suspicious lesions and give these a PI-RADS score”
Advanced multiparametric MRI helps clinicians boost prostate cancer diagnosis
Dr. Steiner explains that techniques for prostate imaging and cancer diagnosis have not changed substantially in the past 30 years, despite the known limitations. PSA testing alone is usually insufficient and current TRUS biopsy techniques often miss anywhere from 40 to 50% of the gland [2]. “PSA testing is imprecise and has a significant number of false positive as well as false negative tests,” he says. “It is, however, the accepted first path of entry for most patients that are ultimately diagnosed with prostate carcinoma.”
The use of MRI has significantly improved capabilities in prostate cancer diagnosis, according to Dr. Steiner. “Multiparametric prostate MRI allows us to look at three parameters to build our diagnosis on: conventional T1 and T2 signal intensity, diffusionweighted imaging and ADC map, as well as dynamic flow imaging, to define the highest probability of prostate carcinoma.”
The standard PI-RADS system is then used to grade lesions based on the MRI findings. For PI-RADS 1 and 2, clinically significant cancer is (highly) unlikely. Intermediate PI-RADS 3 lesions represent a kind of diagnostic “grey area” – these lesions may become PI-RADS 4 lesions if they demonstrate a fusion restriction and hypervascular tumor flow pattern or depending upon index of suspicion. PI-RADS 4 and 5 lesions have a statistically high chance of being a clinically significant prostate carcinoma and should be biopsied. Once biopsy is performed, the pathologists characterize the biopsy samples with either a Gleason score or an ISUP grade group [3].
Clinical case example:
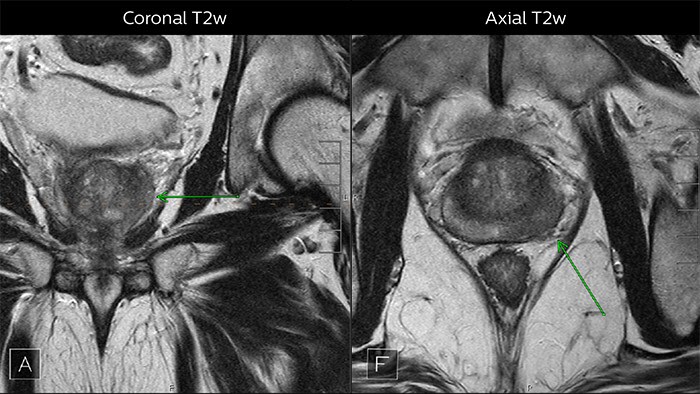
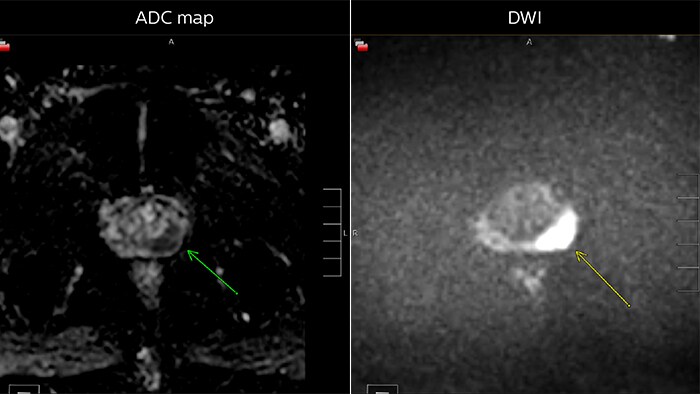
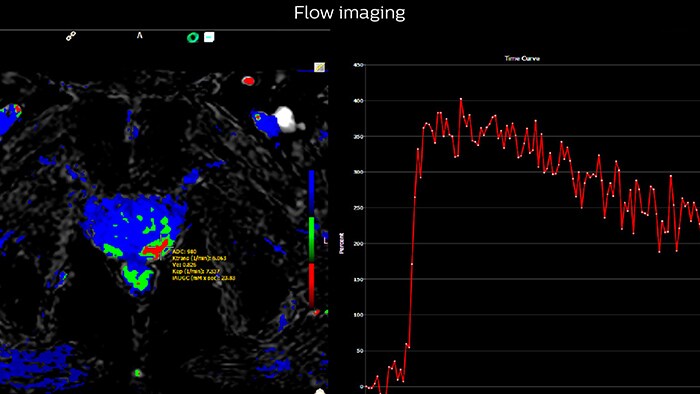
Multiparametric MRI of a classic peripheral zone lesion
For lesions in the prostate’s peripheral zone, the DWI (diffusion weighted imaging) and ADC map are most helpful for our diagnoses. In this case, the DWI shows very bright signal, which indicates diffusion restriction. The arcuate area with significant signal drop out (arrow) on the ADC map is recognized as highly suspect for tumor. On the axial T2- weighted image the capsule contour looks a little irregular (arrow), which we interpret as capsular disruption and I usually give a measurement: this lesion shows larger than 1.5 cm capsular disruption. I don’t see any signs of lymphadenopathy, but interpret this lesion as PI-RADS 5. The hypervascular flow pattern in the bottom images adds to the diagnostic confidence.
")
Predictable MRI patterns help identify suspicious lesions in the whole gland
Depending upon the Gleason score and prior therapies, prostate carcinoma has a certain predictable pattern on multiparametric MRI, according to Dr. Steiner. “In general, lesions in the peripheral zone have decreased T2-weighted signal and are relatively focal,” he says. “In the transitional zone, these lesions are more difficult to evaluate on T1 and T2, but are generally non-encapsulated.”
“We especially look at diffusion-weighted images and the ADC map. Prostate neoplasms generally have diffusion restriction, so they are bright on diffusion-weighted imaging and dark on an ADC map, which is one of the most important characteristics of neoplasms.”
“The third characteristic we look at, flow, is somewhat less specific but may be quite important in deciding whether a lesion is significant or insignificant. Prostate neoplasms often have a hypervascular tumor flow pattern, meaning that there is rapid inflow of blood into the lesion and then rapid outflow due to a disrupted capillary bed. This can be graphed on multi-parametric images, allowing us to define regions of interest and look at the actual flow within these regions.”
“I perform this interrogation using DynaCAD prostate, which also provides an easy way to determine PI-RADS score and create the report for the urologist.”
“In this way, the MRI images can be used for targeting the lesion when performing the biopsy”
Using detailed, segmented MRI images to guide prostate biopsy
Dr. Steiner explains how a “blind” ultrasound biopsy may lead to a negative result, even when a tumor is present. “In a non-targeted biopsy guided by ultrasound, you see the needle and the confines of the prostate, but cannot see the tumor. So, when trying to get 12 cores as evenly distributed as possible, the tumor may still be missed, particularly when it is in the anterior gland, low in the apex or in other regions generally not easily biopsied by ultrasound.”
That is why Dr. Steiner has implemented the pathway where the MRI images can also be used to guide the biopsy. He uses an MR/ ultrasound fusion guided biopsy system, UroNav, which fuses pre-biopsy MRI images of the prostate with real-time ultrasound images during transrectal biopsy, for excellent delineation of the prostate and suspicious lesions, as well as clear visualization of the biopsy needle path.
“I felt strongly that the urologists are used to doing free-hand biopsies – their brain and hand are very used to manipulating the probe,” says Dr. Steiner. “What UroNav offers is no change in that workflow; it takes the diagnostic MRI images and the localized, segmented lesions and adds tracking and navigation to fuse that with the live ultrasound images. In this way, the MRI images can be used for targeting the lesion when performing the biopsy. The UroNav navigation sensor is mounted on the TRUS probe*, so for urologists the manipulation is similar to what they were used to.”
This process allows us to perform focal biopsies of suspicious areas based on PI-RADS categories that indicate the probability of an underlying potential malignancy,” says Dr. Steiner. “As a result of the high confidence gained using this pathway, I have in the meanwhile limited my biopsies to fewer than ten and my goal, as I’m getting more comfortable with the process, is six or less,” he says.
“This process allows us to perform focal biopsies of suspicious areas based on PI-RADS categories that indicate the probability of an underlying potential malignancy”
“We generate over 4500 images per case. Not utilizing an automated process would make interpretation quite difficult”

From MRI to lesion segmentation to biopsy – an efficient process
For Dr. Steiner, DynaCAD is essential as a diagnostic tool for the interpretation of multiparametric prostate MRI. “I have a custom layout that I’m comfortable with; it allows me to link all of the images and shows the T1, T2, diffusion-weighted images and ADC map on one screen. It also shows me the flow patterns on a second screen so that I can actually cross-link and read all of the images at the same time; I just scroll through the depth of the image,” says Dr. Steiner. “DynaCAD also has a PI-RADS module and I can actually annotate anything I dictate and have that as a report to show to the patient or the urologist.”
“We generate over 4500 images per case. Not utilizing an automated process would make interpretation quite difficult. Most people interpret prostate MRIs in a zonal manner, so we need a program such as DynaCAD that allows us to look at the flow pattern in basically one dataset.”
If a urologist determines that a biopsy is necessary, Dr. Steiner uses the DynaCAD segmentation tool to define the prostate contour and the suspicious lesions in 3D. “This data is then sent to the UroNav and my technologist literally combines the realtime ultrasound image with the MRI data, so that the actual MR image is the live image that I’m seeing during the biopsy,” says Dr. Steiner. “Using UroNav, I can get a small lesion that requires biopsy. Performing this is quite like conventional ultrasound-guided transrectal biopsy; quite rapid, and to me, preferable over other methods. Biopsies take approximately 20 to 30 minutes”
“DynaCAD also has a PI-RADS module and I can actually annotate anything I dictate and have that as a report to show to the patient or the urologist”
Diagnostic results driving the use of fusion biopsies
Three years ago, Dr. Steiner found that urologists were still to be convinced of the value of MRI, and he made this his mission. He moved the prostate MRI to 3.0T and introduced the latest software level for both MRI and DynaCAD.
“Change often comes slowly, and positive results are really the only way we could implement change,” he says. “I initially lectured to regional urologists and radiation oncologists and asked them to send me a few challenging patients that had prior negative biopsies, but a high clinical suspicion of prostate carcinoma. Invariably, MRI findings and fusion biopsy led to immediate positive diagnosis of prostate carcinoma in this select population. That’s how we built up confidence. What happened is that the urologists then asked us to perform fusion biopsies on many of their patients.”
“I partnered with one of our local urology groups and we jointly did the first ten MRI fusion biopsies in our operating room, which gave us both experience as well as leadership. Having the UroNav capability added ‘GPS navigation’ to the urologist’s normal workflow and we could perform targeted biopsy. And I already owned DynaCAD, from which data could directly be imported to UroNav. It was a great win-win.”
“DynaCAD allows me to easily import the images into UroNav for eventual biopsy,” he says. “The decision for biopsy is taken after interpreting the MRI. So, if I don’t use DynaCAD/UroNav I would have to import the data into another modality and literally need redo all of my work. That’s exactly what we did in my prior practice. No one liked to do it because of wasted time and there is reimbursement for one interpretation only.”
According to Dr. Steiner, the adoption of MRI fusion biopsies came after several positive prostate cancer diagnoses using their new approach. “In our first 13 cases of repeat fusion biopsy following negative TRUS biopsy, 11 patients yielded positive tissue for clinically significant carcinoma; 92% of 48 targeted cores were positive in PI-RADS 4 and 5 lesions. The entire procedure takes less than 20 to 30 minutes and patients who have previously experienced a conventional transrectal ultrasound-guided biopsy often remark at how easy this procedure is.”
“Since urologists were more likely to send patients to an interventional radiologist, we developed a solid referral base, since York Hospital was a Regional Medical Center,” says Dr. Steiner. “ I still work very closely with my initial urology colleagues and do all of their interpretation and segmentation, thus making this a mutually beneficial and noncompetitive environment.”
“In our first 13 cases of repeat fusion biopsy following negative TRUS biopsy, 11 patients yielded positive tissue for clinically significant carcinoma”
“Change often comes slowly, and positive results are really the only way we could implement change”
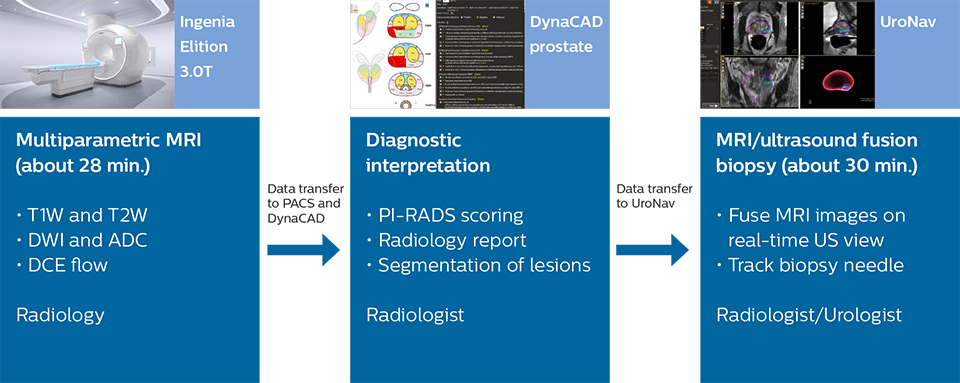
The alternative patient pathway for prostate cancer diagnosis:
Multiparametric MRI and MRI/ultrasound fusion biopsy
")
“We have been reimbursed for this entire procedure. When we can perform three to four biopsies a day, then our break-even is really rapid”
Financial and health-related value associated with fusion biopsy procedure
According to Dr. Steiner, the MRI and fusion biopsy now have proven value. “I believe that utilizing these fusion biopsies in a problemsolving role and in selective patients has been incredible for our community. Patients with clinically significant prostate carcinoma that have had multiple negative biopsies get an immediate diagnosis, go to therapy, and can be potentially cured if they have confined disease. This fact alone saves lives and saves healthcare dollars.”
On the financial aspect, Dr. Steiner explains: “In South Central Pennsylvania, we have been reimbursed for this entire procedure: the diagnostic MRI, secondary segmentation charge prior to fusion biopsy, the technical and professional component of the biopsy, as well as reimbursement for anesthesia and OR time.”
Initially the hospital started with leasing the equipment which has allowed to quickly break even regarding costs, according to Dr. Steiner. “The lease is very beneficial because it allowed us to get started with this procedure that involves both radiology and urology. We started clustering cases, because we’re leasing the equipment per day. I have booked OR time up to twice a week and urologists also have the same OR time, so when we can perform three to four biopsies a day, then our break-even is really rapid.”

Financial and health-related value associated with fusion biopsy procedure
According to Dr. Steiner, the MRI and fusion biopsy now have proven value. “I believe that utilizing these fusion biopsies in a problemsolving role and in selective patients has been incredible for our community. Patients with clinically significant prostate carcinoma that have had multiple negative biopsies get an immediate diagnosis, go to therapy, and can be potentially cured if they have confined disease. This fact alone saves lives and saves healthcare dollars.”
On the financial aspect, Dr. Steiner explains: “In South Central Pennsylvania, we have been reimbursed for this entire procedure: the diagnostic MRI, secondary segmentation charge prior to fusion biopsy, the technical and professional component of the biopsy, as well as reimbursement for anesthesia and OR time.”
Initially the hospital started with leasing the equipment which has allowed to quickly break even regarding costs, according to Dr. Steiner. “The lease is very beneficial because it allowed us to get started with this procedure that involves both radiology and urology. We started clustering cases, because we’re leasing the equipment per day. I have booked OR time up to twice a week and urologists also have the same OR time, so when we can perform three to four biopsies a day, then our break-even is really rapid.”
Rapid scanning time and more patient comfort with Elition
Dr. Steiner currently performs all prostate MRI examinations on the Ingenia Elition 3.0T scanner. “Previously, our scans were over 45 minutes per patient. However, with Elition and Compressed SENSE we have now decreased our scanning time to approximately 25 to 28 minutes, with more patient comfort,” says Dr. Steiner. “We have also achieved significantly improved resolution and more consistent parameters for interpretation. VitalEye, VitalScreen and other workflow features all add significantly to the patient experience as well as patient throughput.”
“With Elition and Compressed SENSE we have decreased our scanning time from over 45 to about 25 to 28 minutes, with more patient comfort”
“One of the big barriers of entry for prostate imaging has been that men do not like the discomfort of a rectal coil. Well, I can say whole-heartedly now, we do not need a rectal coil with our Elition 3.0T system and high quality gradients providing high quality imaging,” says Dr. Steiner. “Additionally, the virtual immersive experience is excellent. Unprecedented comfort and decreased noise are possible.”
“We do not need a rectal coil with our Elition 3.0T system and its high quality gradients providing high quality imaging”
“Many patients have had prior MRIs, which they disliked, because it’s noisy, uncomfortable, boring, and the gantry is tight. And invariably, after we scan them in our Elition, most of them say, ‘Hey, this wasn’t as bad as I thought it was going to be.’ I would say that patients are pleasantly surprised that the scan was quicker than they’ve experienced in the past; the immersive experience is pleasant for them, and the bore seems more open than they remember. The Elition system is definitely a step up in terms of patient comfort and frankly in imaging too.”
When asked if he would recommend 3.0T for prostate imaging, Dr. Steiner says: “Undoubtedly! When I look back at our prior scans that were done on a 1.5T, then the quality, the conspicuity of lesions and my diagnostic confidence are unquestionably improved with the Elition 3.0T. We had looked at all major vendors and selected Philips, because I thought Philips excels in technology as well as the ability to use ExamCards and the ability to cross-train our technologists.”
“I would say that patients are pleasantly surprised that the scan was quicker than they’ve experienced in the past. The Elition is definitely a step up in terms of patient comfort and frankly, in imaging too”
“The combination of MRI and ultrasound fusion biopsy is extremely powerful. We will be doing more and more of these biopsies and scans for the future.”
MRI and MRI-guidance are part of the future of prostate cancer diagnosis
To conclude, Dr. Steiner emphasizes that the power of MRI is now recognized not only for multiparametric examinations to identify suspicious lesions, but also expands into guiding biopsies to inform a definite diagnosis.
“Patients that have PI-RADS 4 and 5 lesions on MRI have a high risk for clinically significant carcinoma. Such lesions are often in the anterior gland, low in the apex, or near regions generally not easily biopsied by ultrasound. These patients now receive MRI/ultrasound fusion biopsies, and this has been our standard of practice now for a year,” says Dr. Steiner. “In my opinion, the combination of MRI and ultrasound fusion biopsy is extremely powerful. We will be doing more and more of these biopsies and scans for the future.”
Summary of Dr. Steiner’s experiences:
References
1. Prostate Imaging Reporting & Data System - PI-RADS 2015 version 2. ACR American College of Radiology. 2. Schouten MG, van der Leest M, Pokorny M, Hoogenboom M, Barentsz JO, Thompson LC, Fütterer JJ. Why and where do we miss significant prostate cancer with multi-parametric magnetic resonance imaging followed by magnetic resonance-guided and transrectal ultrasound-guided biopsy in biopsy naïve men? European Urology;2017;71:896-903. 3. Van Loenhout R, Zijta F, Smithuis R, Schoots I. Prostate Cancer - PI-RADS v2. Radiology Assistant, https://radiologyassistant.nl/abdomen/prostate-cancer-pi-rads-v2
*Contact Philips to ascertain compatibility with your system. PI-RADS® is a registered trademark of The American College of Radiology. Results from case studies are not predictive of results in other cases. Results in other cases may vary.

Subscribe to FieldStrength
Our periodic FieldStrength MRI newsletter provides you articles on latest trends and insights, MRI best practices, clinical cases, application tips and more. Subscribe now to receive our free FieldStrength MRI newsletter via e-mail.
Stay in touch with Philips MRI